How to Build a Healthcare Marketing Strategy That Drives Patient Growth

Ben Henzell
Owner at BFJ Digital

Keep ahead of the curve via our latest trends newsletter.
Contact us nowHealthcare is getting more expensive to market and harder to measure.
Patient acquisition costs are rising as more clinics compete for the same searches. Patient journeys now run across Google (Search, maps, reviews) and, increasingly, AI assistants before anyone calls your front desk. Most providers respond by adding tactics: a new ad campaign. A social push. Maybe even try another agency…
A healthcare marketing strategy is the layer that sits above all of that. It decides which patients are worth acquiring, what you can afford to pay for them, and how your channels work together as a system. Without it, spend leaks, attribution breaks, and your team drowns in admin that produces no bookings.
This blog covers how to build that strategy for the Australian market in 2026. For the channel-level execution that sits underneath it, we have a companion piece on what actually works in healthcare digital marketing. This one is about the thinking that makes those tactics pay.
What a healthcare marketing strategy actually is
Plenty of clinics confuse a strategy with a plan or a channel list. They are different things.
A strategy is a set of commercial decisions. Who is your ideal patient, and which service lines do you want more of? What is a new patient worth, and what can you afford to spend to win one? Which channels advertise which service, and how do they reinforce each other? How will you judge success in bookings and revenue, rather than clicks?
A plan is the calendar and the budget. The tactics are the campaigns themselves. Both depend on the strategy being right first.
Skip the strategy and the symptoms are predictable. You spend across channels with no clear target, so cost per acquisition creeps up. You cannot tell which activity drove a booking, so the budget flows to whatever platform claims the credit. Your team spends hours producing assets and reports that never connect to revenue. The fix is rarely a better tactic. It is almost always a clearer strategy.
Start with the economics, not the channels
Most strategies start with channels. Strong ones start with economics.
Not every patient is worth the same to your business. A single bulk-billed GP visit, a recurring chronic-care patient and a high-margin elective procedure sit at very different points on the value scale. Your strategy should reflect that.
Work out two numbers for each service line. The first is lifetime value (LTV): the total revenue a patient generates across their relationship with you, including repeat visits and referrals. The second is customer acquisition cost (CAC): what you spend on marketing to win one new patient. The ratio between them tells you where to invest and where to stop.
This reframes the whole exercise. A keyword with low search volume can be your most valuable target if it brings in high-LTV patients at a sensible CAC. A high-volume symptom search can be a money pit if it attracts researchers who never book. Demand capture, meaning patients actively searching for your service, usually converts at a lower CAC than demand generation, meaning awareness built before intent exists. Most clinics need both, in a deliberate ratio rather than by accident.
Patient segment | Intent signal | Acquisition cost | Lifetime value | Strategic priority |
High-intent local ("physio near me", "bulk billing GP [suburb]") | Ready to book | Lower CAC | Varies by service | Protect and dominate |
Elective / high-margin (dental implants, allied health programs) | Comparing providers | Higher CAC | High | Invest, with strong conversion and compliance |
Chronic / recurring care | Ongoing need | Moderate CAC | High and recurring | Acquire, then retain through CRM |
Symptom / early research | No booking intent yet | Same click cost, far lower conversion | Low for now | Nurture, do not pay to convert directly |
Referral / word of mouth | Already trusts you | Lowest CAC | High | Systemise reviews and reputation |
Map the channel mix to objective and margin
Once you know which patients you want and what they are worth, the channel mix becomes a budgeting decision rather than a guessing game.
Group your channels by job. Demand capture channels meet patients who are already looking. Organic Search, your Google Business Profile(s) and Google Ads sit here, and they usually deliver the lowest cost per booking. Demand generation channels create interest before the search happens. Social, video and programmatic display sit here, and they protect your future pipeline and your branded search volume.
The mistake is funding one group and expecting it to do the other's job. Pour everything into demand capture and you harvest existing demand until it runs dry, then watch CAC climb as you bid harder for the same finite searches. Pour everything into awareness with no conversion path and you generate traffic that never books.
Allocate to the margin, not the average. The right question is not "what is our blended return", it is "what does the next dollar return in each channel". When an extra dollar in Google Ads returns less than an extra dollar in SEO or retargeting, move it. For the execution detail behind each channel, our healthcare digital marketing work breaks the tactics down by clinic type.
Strategic objective | Primary channels | What good looks like commercially |
Capture high-intent demand | SEO, local SEO, Google Business Profile, booking-intent Google Ads | Low, stable cost per booking; ranking for service and suburb terms |
Build future demand | Meta and social, video, programmatic display | Rising branded search and direct traffic; lower blended CAC over time |
Convert and retain | Website UX, email and SMS, CRM automation | Higher booking conversion rate; more repeat and referral revenue |
Earn trust while patients research | Practitioner content, reviews, AI visibility | Presence in the consideration set before the shortlist forms |
Search is fragmenting, so plan for SEO, AEO and GEO
The biggest shift in healthcare marketing is happening at the discovery layer, and most strategies have not caught up.
Patients no longer start every search on Google's blue links. The same query can now resolve in three different places. A classic organic result. A Google AI Overview that answers without a click. Or an AI assistant such as ChatGPT, Gemini, Perplexity or Copilot, which a patient asks directly: "best physio in Paddington", "is [clinic] any good", "do I need a referral for a dermatologist".
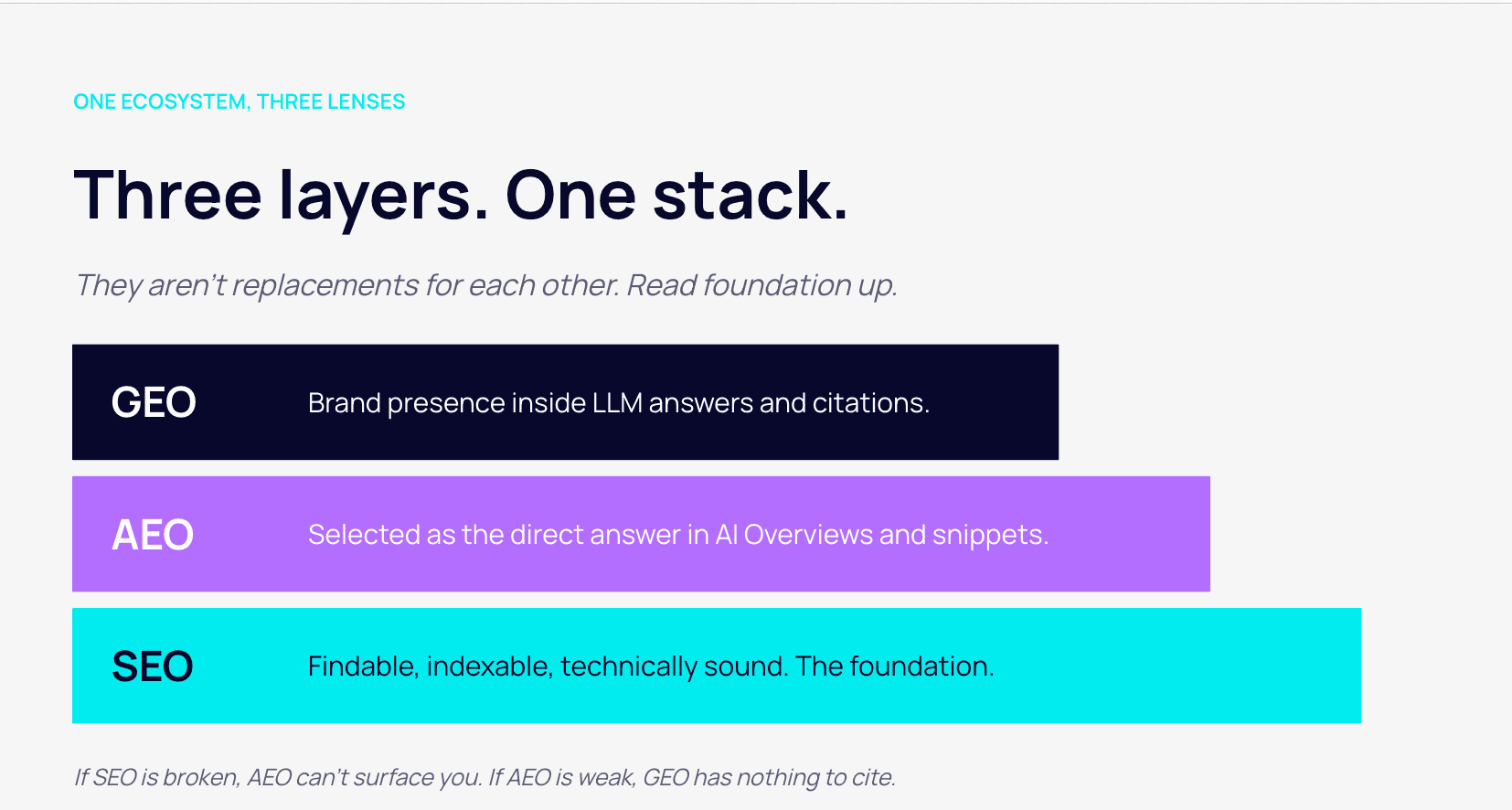
That splits your search strategy into three connected jobs.
SEO, Search Engine Optimisation still earns rankings and clicks for your pages. It remains the foundation.
AEO, Answer Engine Optimisation, gets your content extracted into AI Overviews and featured snippets. It rewards clear structure, direct answers, FAQ schema and unambiguous information about your practice and practitioners.
GEO, Generative Engine Optimisation, is about being mentioned and cited inside the answers that LLMs generate. That depends on demonstrated authority, consistent information about your practice across the web, and content with genuine depth. Thin pages do not get cited.
Healthcare carries extra weight here. Search engines and AI models treat health topics as "your money or your life" content, held to a higher trust bar. Author credentials, clinical review, clear sourcing and a credible practitioner presence all influence whether you surface in Google and in AI answers alike. This is where Google's E-E-A-T framework (experience, expertise, authoritativeness, trust) does real commercial work.
Here is the part most clinics miss. The research phase is moving in front of Google. If an AI assistant does not include you when a patient asks for options, you are out of the consideration set before the shortlist even forms. You will not see it in analytics as a lost click, because there was no click. You will feel it later as rising paid dependence and higher CAC, because the top of your funnel quietly eroded.
You can measure this now. Tracking your brand's mentions and share of voice in AI answers tells you whether you are present in those conversations. Our AEO Audit and the BFJ Labs intelligence platform exist to surface exactly that, and our AEO strategy work turns it into action.
Discovery layer | Where the patient is | What you optimise for | How you measure it |
SEO | Browsing Google results | Rankings and clicks to your pages | Positions, organic traffic, bookings |
AEO | Reading AI Overviews and snippets | Being the extracted answer | Snippet and overview presence, zero-click visibility |
GEO | Asking an AI assistant directly | Being mentioned and cited in the answer | Brand mentions, share of voice in LLMs, citations |
Fix attribution before you scale spend
You cannot allocate a budget well on data that misreports what works. In healthcare, most reporting does.
Healthcare conversions are awkward to track. Many happen on the phone, not a form. Patients research across several visits and devices, then book days or weeks later. Last-click platform reporting credits the final touch, usually a branded search or a retargeting ad, and quietly takes the credit for demand that other channels created.
The commercial cost is real. The budget drifts toward whatever is easiest to measure, not what is most effective. You over-invest in the channels that claim conversions and starve the ones that generate them, which lifts CAC across the board.
A workable measurement model for a clinic connects four things: GA4 with consent mode for on-site behaviour, call tracking to attribute phone bookings to their source, a CRM such as HubSpot to link a first enquiry through to a booked and attended appointment, and offline revenue attribution to tie that appointment back to spend. Built properly, every dollar becomes accountable to a booking and the revenue behind it.
One more shift to plan for. As third-party cookies and cross-site tracking degrade, first-party data becomes your most durable marketing asset. Consent-based email lists, CRM records and your own analytics will outlast the tracking that used to do this job. Building that data now is a strategic decision, not a technical afterthought.
Build compliance into the strategy, not the sign-off
In healthcare, compliance is a design constraint, not a final review. The rules shape which channels you can use, how you target, what you can claim and how you handle data. Bolt them on at the end and you pay for rework, delays and risk.
Three regimes matter most for Australian providers.
AHPRA advertising guidelines govern advertising of a regulated health service across your website, ads, social and newsletters. Testimonials about clinical care are restricted under the National Law, which catches reviews you choose to republish in your own advertising.
The TGA advertising code governs how therapeutic goods and treatments are advertised. Unsubstantiated outcome claims and guarantees are not permitted.
The Privacy Act, overseen by the OAIC, governs how you collect and use sensitive health information. This directly affects email consent, audience building and remarketing. Google also restricts remarketing that segments users by health condition, which limits how you can structure paid audiences.
The strategic implication is straightforward. Compliance narrows your options before the campaign starts, so it belongs in the brief. A specialist plans creative, targeting and data handling within these limits from day one. This is general information, not legal advice.
Confirm specifics with AHPRA, the TGA and your own adviser before publishing.
Regime | What it governs | Strategic implication |
AHPRA advertising guidelines | Advertising of regulated health services, including testimonials | Limits review use and clinical claims across owned and paid content |
TGA advertising code | Therapeutic goods and treatment claims | No guaranteed outcomes; claims need substantiation |
Privacy Act / OAIC | Collection and use of sensitive health data | Shapes consent, email lists and first-party data design |
Platform policy (e.g. Google) | Health-condition targeting and ad formats | Restricts remarketing audiences and some ad types |
The strategic mistakes that cost the most
Most underperformance is structural, not creative. These patterns quietly cost the most.
Running tactics with no strategy. Channels get added one at a time with no shared target. The result is duplicated spend, no clean attribution, and a team buried in admin that never ties back to a booking.
Optimising to last-click. Reward the final touch and you defund the demand generation that fills the top of the funnel. CAC looks fine for a quarter, then climbs as the pipeline thins.
One campaign across every location. Multi-site clinics running a single campaign end up bidding against themselves, cannibalising performance between sites and inflating their own cost per click.
Ignoring AI visibility. Clinics that treat SearchGPTs and AI Overviews as someone else's problem lose the research phase silently, then blame the paid channels that pick up the slack at a higher cost.
Chasing content volume. Publishing more shallow pages does nothing for rankings or AI citations. It adds production cost for assets that never earn their place. Useful content with depth is what gets surfaced.
Treating compliance as a final check. Late AHPRA or TGA issues mean reworked creative, delayed launches and, at worst, takedowns and penalties.
Where to start
For most providers, the priority is sequence over volume. Get the foundations right in this order.
- Map your service-line economics. Establish LTV and a target CAC for each service you want to grow. This anchors every budget decision that follows.
- Fix attribution. Connect analytics, call tracking and your CRM so you can see cost per booking by channel. You cannot allocate well until you can measure honestly.
- Tighten conversion. Make your website and booking flow convert the traffic you already have before buying more.
- Set the channel mix. Split budget across demand capture and demand generation deliberately, and build AEO and GEO into your search plan rather than relying on classic SEO alone.
- Then scale. Once the foundations hold, increase spend in the channels with the strongest marginal return.
Done in this order, your marketing becomes a system you can forecast and control, built around how patients actually research and decide.
Providers that build their strategy around patient economics and real attribution, rather than platform-reported clicks, will hold lower CAC as competition and AI-mediated search keep rising over the next 12 to 24 months.
If you want a clear read on where your gaps are, the digital marketing maturity assessment is a sensible first step. BFJ Digital works with healthcare providers nationally, from local SEO and paid search for clinic networks like SmartClinics and GP groups like Better Medical, through to offline revenue attribution and AEO strategy.
When you are ready to map yours, get in touch.
FAQs: Healthcare Marketing Strategy
What is a healthcare marketing strategy?
It is the set of commercial decisions that sit above your campaigns: which patients you want, what you can afford to acquire them for, how your channels work together, and how you measure success in bookings and revenue. The campaigns are the execution. The strategy is the thinking that makes them pay.
How is a strategy different from healthcare digital marketing tactics?
Tactics are how you run each channel: the Google Ads structure, the SEO work, the social content. Strategy decides which channels deserve a budget, in what ratio, and why.
How do AHPRA and TGA rules affect a healthcare marketing strategy?
They act as design constraints. AHPRA restricts how you use testimonials and clinical claims. The TGA restricts claims about treatments and therapeutic goods. Both shape your creative and your targeting, so they belong in the brief from the start, not the final sign-off. This is general information, not legal advice.
How do we get our practice mentioned in AI search results like ChatGPT?
Through demonstrated authority, structured and genuinely useful content, consistent information about your practice across the web, and strong E-E-A-T signals such as author credentials and clinical review. You can track your presence with an AEO Audit that measures your brand's mentions and share of voice in AI answers.
How much should a healthcare practice spend on marketing?
There is no fixed percentage worth quoting. Set spend against your economics instead: what a new patient is worth over their lifetime, and what you can afford to acquire one for. That keeps the budget tied to return rather than a rule of thumb.
Why is attribution so hard in healthcare?
Because conversions are phone-heavy, span multiple visits and devices, and are often delayed by days or weeks. Platform reporting credits the last click and undervalues the channels that created the demand. A connected model using analytics, call tracking and a CRM gives you a truer cost per booking.
Ben Henzell
Ben Henzell founded BFJ Digital with a simple belief: great marketing should help businesses genuinely grow, not just look good on paper. With over 20 years in the industry, Ben has seen marketing evolve from billboards and print ads to the complex digital ecosystem we navigate today. That perspective is invaluable.
He's worked across traditional and digital channels, giving him a real understanding of what actually moves the needle for businesses. Ben's approach is refreshingly straightforward—he'd rather have an honest conversation about what will work than oversell a flashy strategy.
His Bachelor of Business in Advertising and Marketing gave him the foundation, but it's the two decades of real-world experience that make him someone clients trust when big decisions need to be made.
At BFJ Digital, Ben has built a team that shares his values: do great work, be honest with clients, and focus on results that matter. If you're looking for someone who genuinely cares about your business success and has the experience to back it up, that's Ben.
Ready to See the Bigger Picture?
Want to understand how your digital and real-world marketing impact each other? Not sure if your CRM is supporting your paid media efforts? Just need some clarity and a clear plan to better ROI? Book your free strategy session today for an in-depth audit and action plan to double your digital marketing ROI.
- Meet with a strategy specialist to build a growth plan
- Increase your media performance by up to 200%
- Improve business efficiencies to increase ROI via automation and increase profit
- We cut to the chase. What digital marketing is actually working?